Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2020.v06i01.004
Year: 2020, Volume: 6, Issue: 1, Pages: 18-20
Case Report
M Khizer Hussain Afroze1, M Sangeeta2, Suman Tiwari3
1Assistant Professor, Department of Anatomy, MVJ Medical College and Research Hospital, Bengaluru, Karnataka, India,
2Professor and Head, Department of Anatomy, MVJ Medical College and Research Hospital, Bengaluru, Karnataka, India,
3Associate Professor, Department of Anatomy, MVJ Medical College and Research Hospital, Bengaluru, Karnataka, India
Address for correspondence:
Name: Dr. M Sangeeta, Department of Anatomy, MVJ Medical College and Research Hospital, Hoskote, Bengaluru, Karnataka, India. Phone: +91-9731936362. E-mail: [email protected]
Variations in the pectoralis major (PM) muscles have been reported by various authors in the literature. We report a case of accessory slip of PM with variation in insertion which has not been reported in the literature to the best of our knowledge. This accessory slip was partially muscular getting inserted into medial lip of intertubercular sulcus (ITS) and partially aponeurotic getting inserted into lateral lip ITS, thus forming “H”-shaped pattern. Knowledge of such anatomical variation will create awareness among surgeons performing surgical reconstruction using PM muscle.
KEY WORDS: Chondroepitrochlearis, costoepitrochlearis, pectoralis major
The pectoralis major (PM) muscle usually originates from medial half of clavicle, sternum, costal cartilages (2nd–6th), and aponeurosis of external oblique. It normally gets inserted into lateral lip of intertubercular sulcus (ITS).[1] Variations in the PM muscles have been reported by various authors in the literature. These variations include chondro- or costo- epitrochlearis muscle, chondro- or costo-humeralis, chondrofascialis, and thoracoepitrochlearis.[2] The present case is a slightly different variation involving insertion of PM which has not been reported in the previous literature to the best of our knowledge.
Such variations are of both academic and clinical interest. Academically, they add to the knowledge of existing literature and clinically they are imperative during surgical reconstruction involving axilla and breast. Radiologist should be aware of this variation because abnormal muscles may mimic as soft-tissue tumors in radiograms.[3]
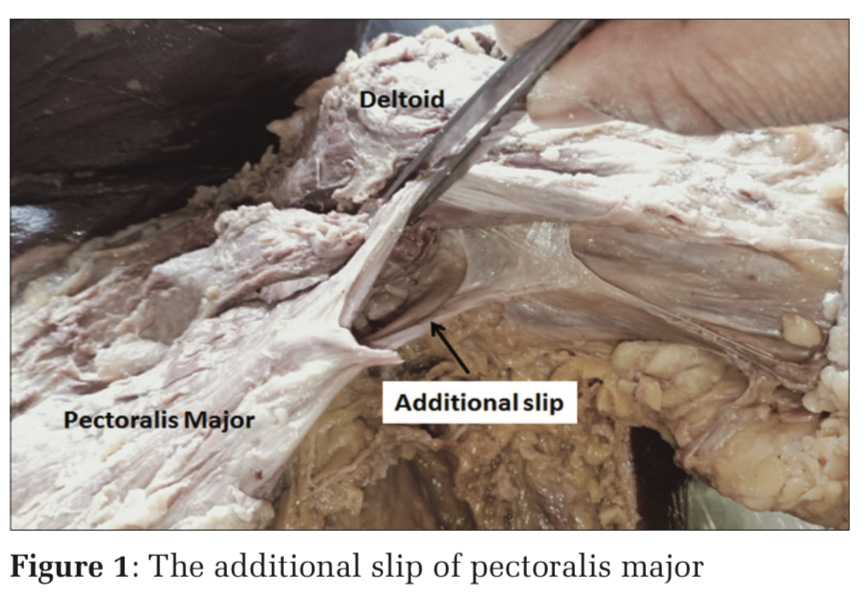
During routine dissection of a 60-year-old female embalmed cadaver in the Department of Anatomy at MVJ Medical College and Research Hospital, we observed a variation in the insertion of PM muscle. The pectoral region was dissected following the steps in Cunningham’s dissection manual. The PM muscle was exposed after removing the skin, superficial fascia, and pectoral fascia. The origin of PM was found to be normal.
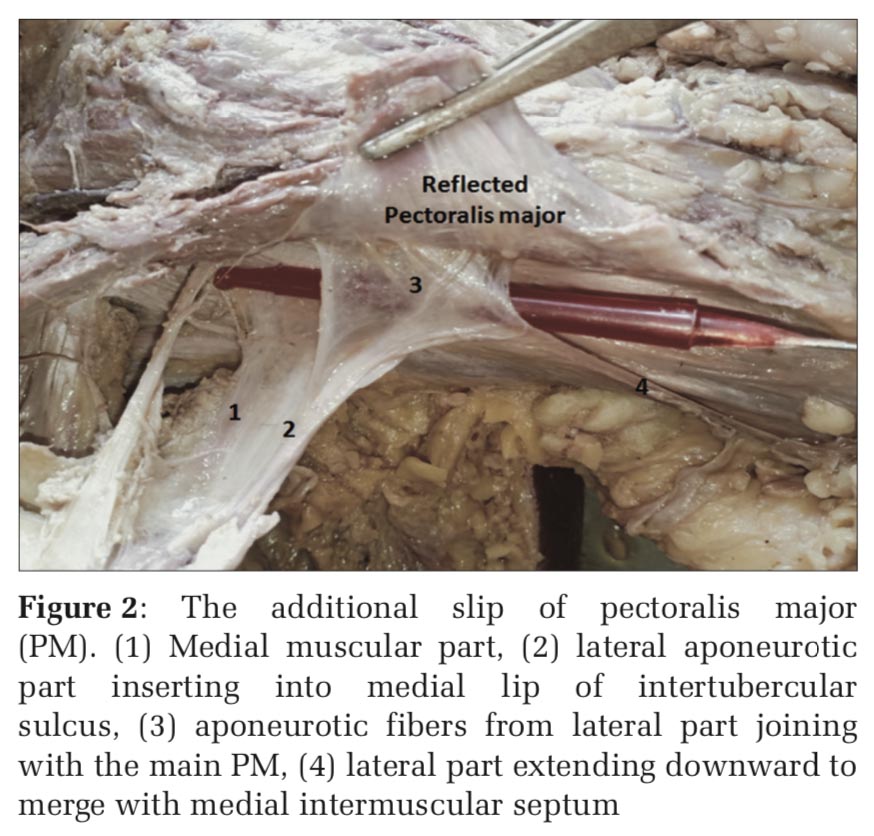
Additional slip of PM was seen arising deep to and from the lower border of PM. This additional slip was partially muscular (medial part) and partially aponeurotic (lateral part). Both the medial muscular part and lateral aponeurotic part were seen getting inserted into the medial lip of ITS. The latter one was extending downward and merging into the upper one third of medial ITS. The aponeurotic fibers which were attached into the medial lip also extended horizontally to the lateral lip of ITS, thereby forming the bridge between the two lips. The additional slip was supplied by a twig from the lateral pectoral nerve (Figures 1 and 2).
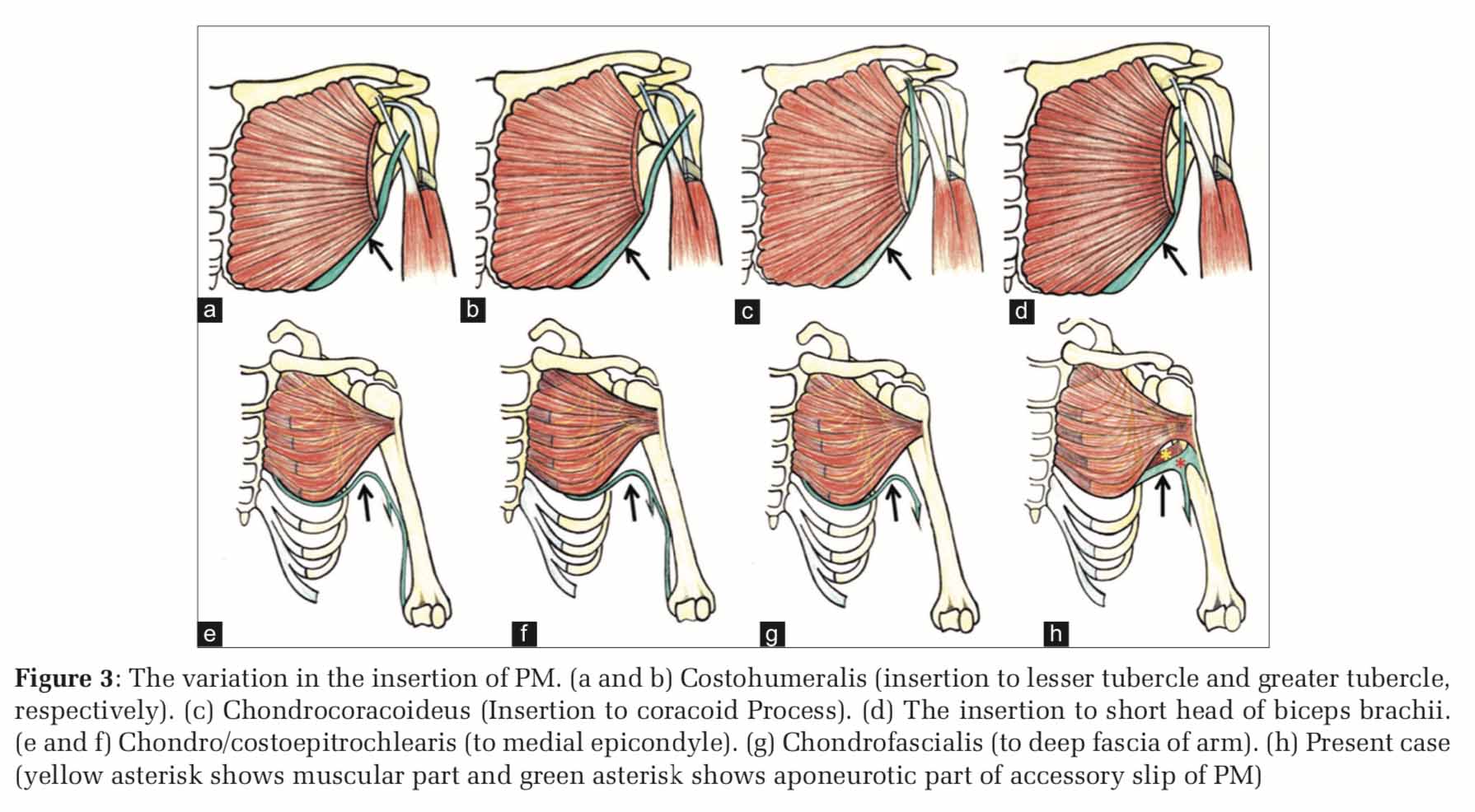
As per review of the literature, the incidence of PM malformations ranges from 0.009% to 0.061%.[4] Many variants of insertion of PM (Figure 3) includes attachment to corocoid process (chondrocoracoideus), into either lesser tubercle or greater tubercle (costohumeralis), into the medial epicondyle (chondroepitrochlearis or costoepitrochlearis), and into the deep fascia of arm (chondrofascialis).[2]
Venieratos et al.[3] reported an accessory left-sided chondrocoracoideus muscle as an extension of abdominal portion of PM. This muscle originated as three slips from 5th to 6th ribs and inserted into coracoid process after fusing with the short head of biceps.
Costohumeralis is a variant of PM arising from 5th to 6th costal cartilage and getting inserted into any part of humerus (lesser or greater tubercle and epicondyle). Rao et al. reported a similar case.[5] Chondroepitrochlearis muscle (CEM) was the term used specifically if the insertion was in the medial epicondyle. CEM as the name implies is a muscle that originates from costal cartilage or costochondral junction and inserts into the distal humerus. This name was first coined by Duvernoy and later modified by Loukas as thoracoepicondylaris which characteristically described its precise insertion into humeral epicondyle.[6] Bilateral CEM was observed by Palagama et al.[7]
Another variant reported by Shetty et al. was the costodorsalis, a muscular slip originating from the sixth rib near the costochondral junction running along the lower border of PM muscle crossing the axilla and merging with the latissimus dorsi muscle.[8]
Pectoralis quartus arises from the 5thto 6th costochondral junction as a separate slip below the pectoralis minor and gets inserted deep to the PM.[9] A complete absence of PM has also been reported by Standring.[10]
Embryologically, pectoral muscles develop from 5th to 7th cervical myotomes during the 5th week of intrauterine life. The abdominal portion is said to be derived from panniculus carnosus which usually regress during evolution and remnants of the same may be seen as extra slips of the PM muscle making this an atavistic anomaly.[2]
Above said variation may present clinically as muscle entrapment causing limited shoulder movement in particular shoulder abduction. It may also present as neurovascular entrapment causing compression of axillary neurovascular bundle. Surgical excision of muscle band would be needed to relieve above symptoms.
Knowledge of variations involving anterior thoracic wall is of paramount importance to surgeons performing axillary lymphadenectomy and breast reconstructive surgeries using PM as a myocutaneous flap. In addition, this variation may also be of academic and clinical interest to radiologists, orthopedicians, and physiotherapists.
Subscribe now for latest articles and news.