Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v10.i1.23.10
Year: 2024, Volume: 10, Issue: 1, Pages: 104-110
Original Article
Tarun Bali1 , Bhavuk Garg2 , R Raghavendran3
1Department of Orthopaedics, East Point College of Medical Sciences and Research Centre, Bengaluru, India,
2Department of Orthopaedics, AIIMS, Delhi, India,
3School of Medical Science and Technology, IIT, Kharagpur, India
Address for correspondence:
Tarun Bali, Department of Orthopaedics, East Point College of Medical Sciences and Research Centre, Bengaluru, India.
E-mail: [email protected]
Received Date:09 December 2023, Accepted Date:08 April 2024, Published Date:27 April 2024
Background: Distal forearm fracture is the most common fracture encountered in daily life. Patients with this type of injury suffer from meaningful pain after Emergency Department discharge. Various studies reported that short-arm, below-the-elbow casts perform as well as long-arm, above-the-elbow casts for maintaining a reduction of distal forearm fractures demonstrated with a comparable risk of complication. Consequently, short casts are the commonly used method of immobilization however, short casts carry a potential disadvantage. Objective: To evaluate the safety and efficacy of the next-generation FlexiOH® (Short Arm Immobilizer). Settings and Design: This is a prospective, multicentre, and open-label clinical trial conducted in 5 different sites in India by recruiting a total of 137 subjects who were presented with distal forearm fractures. Materials and M ethods: Vital signs, concomitant medication taken by subjects during the study, X-ray results, and adverse events caused during all three visits were evaluated. Results: Overall patients showed normal vital signs, minimal adverse events, and relatively less concomitant medication consumption during the study period and at the end of the study, 100% healing was noted among all the study participants in the X-ray investigation. This clearly demonstrates the benefits over the conventional methods. Conclusion: For uncomplicated care of fractures and sports injuries of the limbs, FlexiOH® (Short Arm Immobilizer) technology offers more than just reliable immobilization and has advantages over contemporary plaster and cast bandages. This product is the most advanced orthopaedic immobilization technology and has the potential to be used and adopted worldwide.
Keywords: FlexiOH®, Distal radius fractures, Short arm immobilizer, Adverse events
Distal radius fractures (DRFs) are the most common clinical challenge encountered during orthopaedic trauma care. Conventionally, immobilization includes that the elbow would ensure better control of fracture instability, preventing loss of reduction which results in better clinical outcomes. Initial treatment usually consists of closed reduction and splint immobilization 1, 2 followed by surgical reduction if the closed manipulation is not acceptable 3, 4, 5 . If, however, there is a stable fracture pattern and acceptable alignment, then casting may prove to be satisfactory. In a long-arm cast, non-operative immobilization is generally maintained 6, 7 . This prevents elbow motion and forearm rotation, which theoretically minimizes the risk of fracture displacement 8 . Nevertheless, even for unstable fractures, some surgeons choose a short arm cast 2, 9 . Long arm casts are cumbersome; however, the patients generally find treatment with lighter short arm casts is relatively more comfortable.Presently, there is no agreement on the most effective method for immobilizing a DRF. There have been several methods discussed, but none have been identified to be more efficient than the others 1, 10, 11, 12 . As per the clinical practice guidelines from the American Academy of Orthopaedic Surgeons, the evidence for and against elbow immobilization in patients undergoing cast treatment is "inconclusive" and the choice between both of them is left to the clinician's discretion 13. The hypothesis in many studies of which short arm casts may perform as well as long arm casts to maintain the reduction of DRFs has been examined. Casting applied too tightly can lead to compartment syndrome, impairing circulation and producing local nerve damage. Skin ulcers can be produced if local pressure over the skin is not avoided with adequate padding, over bony prominences. Joint stiffness of the hands and fingers can be produced with prolonged forearm casting 14 .
The FlexiOH® (short arm Immobilizer) is a next-generation orthopaedic immobilization technology that is completely washable and made of an innovative, light-curing mesh material that is easy to fix and wearable on the fractured part, providing rigidity for supporting the fractured part while also ensuring proper skin hygiene. The cast is easy to put on, quickly closed with the zipper, and hardens in a few minutes, is also 100% waterproof and provides 46% exposed skin area. FlexiOH® (short arm Immobilizer), unlike conventional plasters and casts, also is simple to use while washing, taking a shower, or even swimming. Itchy, hard-to-reach areas are also a thing of the (plaster) cast. The immobilization technology of FlexiOH® is thus an air-permeable and waterproof alternative to classic plaster casts. With this background, this study was conducted to determine the safety and efficacy of FlexiOH® (short arm immobilizer) in the treatment of DRFs, this would be as effective as conventional casts and plasters.
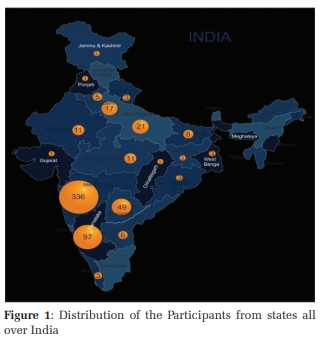
A prospective, multicentric, and open label clinical study was conducted to evaluate the safety and efficacy of FlexiOH® (Short Arm Immobilizer) in the treatment of DRFs. The study included data for safety and efficacy analysis from 5 different sites across India and the study was approved by the respective ethics committee.
Male or female aged 18 to 80 years (both inclusive).
Subjects who belong to the following AO classification having closed fractures of the distal end of the radius or/and the ulna and who do not need either internal or external fixation of the fracture.
Distal Radius Fracture:
Extraarticular
Radial styloid avulsion
Simple
Distal Ulnar Fracture:
Styloid Process
Simple
Radiological features following the above AO classification.
Pre-operative or Post-operative stabilization.
Subjects with the absence or presence of any of the following sprain of the ligament around the wrist which does not require operative treatment and require below elbow cast application.
Collateral ligament injury of the wrist
Carpal ligament injury of the wrist
Ligament injury of distal radio ulnar joint
Instability of distal radio ulnar joint
Carpal instabilities
Radio Carpal ligament injury
Undisplaced scaphoid fracture
Undisplaced lunate bone fracture
Other carpal bone fracture
Subjects who gave written informed consent.
Presence of wound involving deeper tissues or requiring suturing.
Ulceration or any skin conditions present that may interfere with the study.
Open wound aligns with fracture, fracture requires internal fixation.
Subjects scheduled for surgical management. Subjects with other comorbid conditions, such as osteomyelitis, severe dementia, or rheumatoid arthritis.
Known skin allergy and skin disease.
Mentally challenged subjects.
Subjects refused to give written informed consent.
A total of 137 subjects from 5 different sites across India i.e., 24 subjects from the 1st centre, 21 subjects from the 2nd centre, 18 subjects from the 3rd centre, 17 subjects from 4th centre and 57 subjects from the 5th centre were involved. On the patient’s hand, the FlexiOH® short arm immobilizer was applied using a zip and then cured using the Rizycure® light device which was recommended for the duration of 3-20 minutes based on the size of the immobilizer. (Figure 1) When it became rigid, the zip puller was cut using pliers so that the patient could not take off the immobilizer on their own.
The patients were followed, and the data were recorded at visit 1(screening visit), visit 2, and visit 3. The data recorded were the vital signs - systolic blood pressure (SBP), diastolic blood pressure (DBP), temperature, pulse rate, X-ray results, concomitant medication prescribed for the subjects during the study, and any adverse events caused during all three visits. Data was collected and entered in the predesigned Excel spreadsheet and were presented in the form of frequencies and percentages.

Systolic Blood pressure (SBP) of all 137 subjects were ranging from 100-142 mmHg in all the 3 visits. SBP among patients varied significantly in a few patients but was considered normal, whereas the Diastolic Blood Pressure (DSP) showed values between 60 to 92 mmHg in all three visits. The temperature and pulse rate of subjects ranged from 35 °C to 37 °C and 60 to 94 bpm, found normal throughout the study. SBP, DBP, temperature, and pulse rate showed normal throughout the study during all 3 visits.
Out of 137 (100%) subjects, wrist stiffness was reported in 27 (20.33%) subjects, followed by distal Oedema in 24 (17.5%) subjects, followed by muscular atrophy in 8(5.8%) and only 2(1.5%) patients reported skin infections during the study. These are expected AEs due to the immobilization and we report that it is very minimal compared to the conventional one. X-ray was done for Visit 1 and Visit 3 and analyzed for all the subjects. X-ray results showed that the study subjects were completely healed on the 3rd visit. FlexiOH® (Short Arm Immobilizer) was very effective as 100% of subjects showed healing complete on the 3rd Visit (Table 1 and Figure 2) and satisfactory range of motion after removal of FlexiOH® (Figure 3).
|
|
Visit 1 (n=137) |
Visit 3 (n=137) |
|
Healing Complete |
0 |
137 (100%) |
|
2nd MC shaft fracture (LT) |
3 (2.2%) |
0 |
|
3rd MC shaft fracture (LT) |
4 (3%) |
0 |
|
3rd, 4th, 5th MC base fracture (RT) |
2 (1.5%) |
0 |
|
4th, 5th MC base fracture (RT) |
2 (1.5%) |
0 |
|
5th MC shaft fracture (RT) |
6 (4.4%) |
0 |
|
Chauferrs fracture (LT) |
4 (3%) |
0 |
|
Distal radius & ulna fracture (LT) undisplaced |
10 (7.3%) |
0 |
|
Distal radius & ulna fracture (RT) |
3 (2.2%) |
0 |
|
Distal radius and ulna fracture (RT) undisplaced |
5 (3.6%) |
0 |
|
Distal radius fracture (LT) |
4 (3%) |
0 |
|
Distal radius fracture (RT) |
5 (3.6%) |
0 |
|
Distal radius hairline fracture (LT) |
3 (2.2%) |
0 |
|
Distal radius hairline fracture (RT) |
2(1.5%) |
0 |
|
Distal radius with intraarticular ex fracture (RT) |
4(3%) |
0 |
|
Distal ulna fracture (LT) undisplaced |
2 (1.5%) |
0 |
|
Distal ulna fracture (RT) |
6 (4.4%) |
0 |
|
DRUJ sprain (LT) |
2 (1.5%) |
0 |
|
DRUJ sprain (RT) |
2 (1.5%) |
0 |
|
Impacted scaphoid fracture (LT) |
2 (1.5%) |
0 |
|
Impacted scaphoid fracture (RT) |
3 (2.2%) |
0 |
|
Radius styloid fracture (RT) with minimal displacement |
2(1.5%) |
0 |
|
Scaphoid fracture (LT) undisplaced |
3 (2.2%) |
0 |
|
Ulna styloid fracture with minimal displacement |
2 (1.5%) |
0 |
n = Total number of subjects, % = Subjects with particular fracture / n


All 137 subjects were on concomitant medication in the first visit for pain and inflammation management. Most of the study subjects were prescribed diclofenac 95 (69.3%) in the 1st visit followed by Etoricixib in 113 (82.5%) and Paracetamol in 116 (84.7%) in the second visit and third visit respectively. We observed that at the end of the study, there was a decrease in the requirement of concomitant medication for the management of pain which is comparable to the baseline (Table 2).
|
Medications |
Visit 1 (n=137) |
Visit 2 (n=137) |
Visit 3 (n=137) |
|
No Concomitant Medication |
0 |
2 |
7 |
|
With Concomitant Medication |
137 (100%) |
135 (98.5%) |
130 (94.9%) |
|
Drug Name |
|||
|
Aceclofenac |
0 |
2 (1.5%) |
0 |
|
Aceclofenac & Paracetamol |
11 (8.0%) |
4 (3%) |
3 (2.2%) |
|
Aceclofenac & Paracetamol, Pantaprazole & Domperidone |
1 (0.73%) |
0 |
0 |
|
Aceclofenac & Paracetamol, Trypsin Chymotrypsin |
2 (1.5%) |
2 (1.5%) |
1 (0.73%) |
|
Aceclofenac & Paracetamol, Trypsin Chymotrypsin, Pantoprazole & Domperidone |
1 (0.73%) |
0 |
0 |
|
Calcium citrate, Malate, Vitamin D3 & Folic Acid |
0 |
1 (0.73%) |
0 |
|
Calcium citrate, Malate, Vitamin D3 & Folic Acid, Etoricoxib, Paracetamol |
1 (0.73%) |
0 |
0 |
|
Diclofenac |
95 (69.3%) |
0 |
0 |
|
Diclofenac, Pantaprazole |
1 (0.73%) |
0 |
0 |
|
Etoricoxib |
0 |
113 (82.5%) |
4(3%) |
|
Etoricoxib & Paracetamol |
13 (9.5%) |
7 (5.1%) |
3(2.2%) |
|
Etoricoxib & Paracetamol, Hydroxyzine Hydrochloride |
0 |
1 (0.73%) |
0 |
|
Hydroxyzine |
0 |
1 (0.73%) |
1 (0.73%) |
|
Hydroxihydroxyzine |
0 |
0 |
1 (0.73%) |
|
Hydroxyzine Hydrochloride |
0 |
2 (1.5%) |
0 |
|
Hydroxihydroxyzine Hydrochloride |
0 |
1 (0.73%) |
0 |
|
Hydroxihydroxyzine & Etoricixib & Paracetamol |
0 |
1 (0.73%) |
0 |
|
Naproxen Sodium, Domperidone |
12 (8.8%) |
0 |
1 (0.73%) |
|
Paracetamol |
0 |
0 |
116 (84.7%) |
Overall, in the present study, the vital signs, adverse events, and concomitant medication showed normal results with minimal adverse events. The X-ray findings showed that the fracture in all 137 subjects completely healed at 3rd visit. With these promising results, we claim that FlexiOH® technology offers more than just reliable immobilization for uncomplicated care of fractures and sports injuries of the limbs. As a contemporary alternative to plaster and cast bandages, the flexible and slightly stretchable plastic material fits snugly around the arm and can be easily closed with the integrated zipper. After the treatment duration, the splint can be rapidly and painlessly removed by opening it up once more. FlexiOH® is a waterproof and breathable cast that allows you to shower, swim, and carry out daily activities without damaging the cast or compromising hygiene. The waterproof feature enhances convenience and helps maintain better skin health by preventing moisture accumulation and associated problems like maceration and foul odour. The breathability of this cast also helps with air circulation, reducing the likelihood of skin irritation and providing a more comfortable healing experience.
Casting does have some risks and it is inevitable sometimes. Firstly, because of immobilization, some of the complications such as thrombosis, muscle atrophy, joint stiffness, and disuse syndrome were reported. Secondly, conventional casts have certain specific complications. The most reported ones include a limited blood supply when the cast is applied too tightly or otherwise gets too tight due to swelling, acute compartment syndrome, and compression neuropathy 15 . The six P's are used to describe the first complication, acute limb ischemia: pain (typically in the distal region of an extremity), poikilothermia (sensation of cold on the skin), pallor, pulselessness, paresthesia, and paralysis 16 . Due to compression neuropathy, nerve conduction is delayed and eventually completely inhibited when ischemia occurs. Weakness and pain are symptoms 17 . Compartment syndrome is the third and most significant complication with the conventional cast. Compartments in the limbs are divided by strong, fascial membranes and contain muscle groups. Compartment syndrome develops when a compartment's pressure rises and compromises the circulation as well as the function of the compartment's contents 18 . Pain is the most significant symptom. Compartment syndrome is associated with pain that causes a burning sensation, appears after a delay of time, aggravates more severely, or occurs when a passive stretch is applied to the compartment. Paralysis and paresthesia are other symptoms; however, they appear later.
Although the pressure in the compartment is generally lower than the systolic blood pressure, the presence of arterial pulses does not exclude the diagnosis of compartment syndrome. In addition, the tissue may appear noticeably swollen and may feel tense to palpation 19 . In addition to these complications, conventional casts have some practical limitations that may affect the patient's quality of life, and these include sweating, having to carry around a lot of weight, as well as not being able to take a shower. Also, when there is a requirement for an examination or x-ray, the cast must also be entirely removed as well as changed. These difficulties can be resolved by using a short arm immobilizer device from FlexiOH® because they are up to 50% lighter than a conventional cast, waterproof, provide aeration, and are simple to use and take off Without having to make use of any other external cast cutter/spreader, FlexiOH® can be removed following the course of treatment. FlexiOH® is carefully engineered using materials and a design that is meant to give the patient the best possible comfort. Foam that comes into contact with the skin is biocompatible (certified by ISO 10993-10) and offers protection from the hardened polymer. The intermittent hollow spaces in the FlexiOH® short arm immobilizer are designed to make it more convenient for air to circulate and for water or sweat to evaporate from the skin's surface. The radiolucency property of FlexiOH® short arm cast does not interfere with the radiological imaging or diagnosis. Because of all these advantages and promising study outcomes, we recommend that surgeons utilize FlexiOH® short arm immobilizer can be a potential solution in treating patients with distal radius fractures patients.
FlexiOH® is a new revolutionary orthopaedic immobilization device that can be applied for both bone fractures as well as musculoskeletal injuries and offers a safe alternative over the conventional cast, which has major side effects. It is affordable and can easily be available depending on the size and variant of the cast needed. The product is the most advanced orthopaedics immobilization technology and has the potential to be used and adopted throughout the world.
Subscribe now for latest articles and news.