Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v9i1.22.244
Year: 2023, Volume: 9, Issue: 1, Pages: 29-36
Original Article
J Sriharsha1 , S B Adarsh1 , Madhu Srinivasarangan2 , S Ruben Omar3
1Assistant Professor, Department of Emergency Medicine, JSS Medical College and Hospital, Mysuru, 570004, Karnataka, India,
2Associate Professor, Department of Emergency Medicine, JSS Medical College and Hospital, Mysuru, 570004, Karnataka, India,
3Senior Resident, Department of Emergency Medicine, JSS Medical College and Hospital, Mysuru, 570004, Karnataka, India
Address for correspondence:
S Ruben Omar, Senior Resident, Department of Emergency Medicine, JSS Medical College and Hospital, Mysuru, 570004, Karnataka, India.
E-mail: [email protected]
Received Date:19 July 2022, Accepted Date:06 December 2022, Published Date:13 January 2023
Introduction: Rapid Sequence Intubation (RSI) is the definitive modality of airway management when resuscitating trauma patients in the Emergency Department (ED). This study was done to evaluate the utility of POCUS in RSI and its efficacy in confirming tube placement as compared to conventional methods. Aims & Objectives: Primary Objectives - Time taken for airway evaluation and identifying potentially fatal conditions using POCUS guided Intubation Algorithm (PA) during RSI. Proper placement of the endotracheal tube and confirmation of the same was also assessed and compared with the conventional technique. Methodology: A prospective, randomized single-centred study was conducted in 100 trauma patients requiring emergent airway management, presenting to the ED. The time taken and efficacy of confirmation of tube placement is recorded and compared in two arms. Results: In our study we found the mean procedure time for ETT placement was less in the PA arm compared to the CE arm (45 vs 91.36 seconds, p<0.0001). Oesophageal intubations were detected in the PA arm in 22 seconds vs 114 seconds in CE arm with a p< 0.0001 and the time taken for effective reintubation was 26.67 vs 55 seconds in the PA and CE arm with a p value < 0.007 respectively. Conclusion: POCUS detected oesophageal intubations and confirmed proper tube position in less time when compared to standard techniques such as five-point auscultation and capnography. The results of this study have proved that POCUS is a useful adjunct to the Emergency physician to improve quality of care in trauma patients.
Keywords: Point of care ultrasound, Rapid sequence intubation, Trauma, Emergency department, Emergency physician, Endotracheal tube, End tidal carbon dioxide, Ultrasound, Clinical examination
The first and the most important task of every Emergency physician is the management of his patient’s "A-B-C"s, i.e. Airway-Breathing-Circulation in that particular order of precedence. It has been found that majority of trauma deaths usually occur within the first hour from the time of occurrence or "the Golden Hour". Hence, any failure to promptly secure an adequate airway in the already compromised trauma victim can accelerate his journey on the road to further morbidity and mortality. Rapid Sequence Intubation is the cornerstone of emergency airway management and it consists of three phases - Preoxygenation, Endotracheal tube placement and Confirmation of Tube Placement. Any delay in the latter two phases lead to compromised patient outcomes. Recent studies have demonstrated the utility of Point of Care Ultrasound [POCUS] in speeding up the process of RSI and at the same time, improving the efficacy of the process. Current systematic reviews have demonstrated its use in excluding oesophageal intubation and in shortening intubation times by a considerable margin. It is also an easy, bedside, highly reproducible means to identify hidden threats to the airway [like tracheal injury, hematoma, and vocal cord palsy] and in breathing [pneumothorax, haemothorax] and to dynamically visualise tube placement with relative
To evaluate the POCUS guided Intubation Algorithm during rapid sequence Intubation in trauma resuscitation by measuring the time taken for correct Intubation and identifying potentially fatal conditions affecting emergency airway management.
To measure the time taken to detect oesophageal intubation.
To measure the time taken to correct oesophageal intubation.
Medical records of patients in the Department of Emergency Medicine, JSS Hospital, Mysuru
Hospital-based prospective study
One year and six months
Purposive sampling. Sample size of 100 patients was used in the analysis, separated into two groups
Any Trauma victim > 18 years of age attending the Emergency Department of JSS Hospital and undergoing Rapid Sequence Intubation (RSI) for airway or breathing management
Patients in cardiac arrest
Overt tracheal injury
Open thoracic wound
Patients requiring surgical airway
Transfer-in patients with an existing endotracheal tube
Pregnant patient (with positive urine on serum β-HCG)
It was proposed to evaluate the integration of POCUS in trauma resuscitation through the use of an algorithmic approach to POCUS during Rapid Sequence Intubation (RSI)
The study subjects were randomly assigned to the Clinical Examination (CE) arm, or POCUS guided Intubation Algorithm (PA) arm. Randomization of the first patient was done by coin toss and the selected patient was allocated into USG arm. Every subsequent patient selected for the study was alternatively allotted to the CE and USG arm. The treating medical team decided on airway management and whether to utilise any other radiological or non-radiological investigations, including ultrasonography; the study will not have any direct or indirect involvement in the management decisions. All the findings were recorded by an observer (emergency nurse/ Emergency Medicine Technician) in the Emergency Department.
In this study, Rapid Sequence Intubation (RSI) were considered in three stages-
Stage 1: The Pre-Oxygenation Stage
Stage 2: Tracheal Intubation, and
Stage 3: Confirmation Stage.
The first stage of pre-oxygenation typically was of 3 minutes in duration. The primary survey in the CE arm involved the medical team to perform a thorough clinical examination and chest auscultation as per the Advance Trauma Life Support (ATLS) guidelines looking for signs and symptoms suggestive of a Pneumothorax, Neck Hematoma and other life-threatening Airway and Breathing injuries. The POCUS-guided Intubation Algorithm (PA) arm performed a primary survey as per the ATLS guidelines utilizing a POCUS guided examination of neck and chest to look for pneumothorax signs, tracheal injury, anticipated difficult intubation, or any abnormal vessels in the neck.
In the second stage, both arms underwent Endotracheal Intubation as per the standard protocol followed. In the CE arm, a five-point chest auscultation method combined with End-Tidal CO2 to confirm the endotracheal tube position as part of the third stage was performed. In the POCUS guided Intubation Algorithm (PA arm), the trained sonographer performed tracheal ultrasound (to look for evidence of Oesophageal intubation) and left lung ultrasound (to demonstrate left side pleural sliding) to confirm the endotracheal tube position. The abnormal POCUS findings were recorded and reviewed by the consultant Emergency Physician after every 10 cases.
The time taken from the start of endotracheal intubation to the confirmation of endotracheal tube placement was recorded by the observer using an electronic stopwatch with multiple laps.
The number of oesophageal intubations, time taken to detect the same in both the arms was also recorded.
The patient’s clinical course in the post-intubation stage was also noted in both the arms.

Data was entered into Microsoft excel data sheet and analysed using SPSS 22 version software.
Categorical data was represented in the form of Frequencies and proportions. Continuous data was represented as mean and standard deviation.
Independent T test was used to check for association between the mean values of variables in both groups of the study. Chi square was used to check for association of qualitative data.
Pearson correlation Test was used to analyse the correlation between continuous variables.
Graphical representation of data: MS Excel and MS word was used to obtain various types of graphs such as bar diagram and Scatter diagram.
|
|
Group |
|||||||
|
POCUS guided Intubation Algorithm (PA) arm. |
CE |
|||||||
|
Minimum |
Maximum |
Mean |
Standard Deviation |
Minimum |
Maximum |
Mean |
Standard Deviation |
|
|
Time Taken for Primary Survey in Sec |
18.00 |
45.00 |
25.16 |
5.36 |
17.00 |
30.00 |
22.16 |
2.94 |
Independent T test = 3.472, p=0.001

This study found that the mean time taken for primary survey was 25.16 ± 5.36 seconds in the POCUS guided Intubation Algorithm (PA) arm versus 22.16 ± 2.94 seconds in the CE arm, with a statistically significant difference between the two (p=0.001).
|
|
Group |
|||||||
|
POCUS guided Intubation Algorithm (PA) arm. |
CE (EtCO2 method) |
|||||||
|
Minimum |
Maximum |
Mean |
Standard Deviation |
Minimum |
Maximum |
Mean |
Standard Deviation |
|
|
Mean Time Till Positive Confirmation Of ET Tube Placement in Sec |
33.00 |
59.00 |
45.00 |
7.83 |
77.00 |
186.00 |
91.36 |
19.63 |
Independent T test = 15.51, p=0.0001

In our study, the mean time taken from the beginning of intubation till positive confirmation of tube placement was significantly lesser in the PA arm when compared with the CE arm (45.00 ± 7.83seconds vs 91.36 ± 19.63seconds, p=0.0001)

The mean time taken to detect oesophageal intubation was 22 ± 2s in the PA arm, as compared to 114 ± 5.65s in the CE arm with a statistically significant difference between the two (p= 0.0001).

Following the detection of oesophageal intubation, the mean time taken for re-intubation was 26.67 ± 3.05s in the PA arm and 55 ± 7.07s in the CE arm and the difference between the two was found to be statistically significant with a p value = 0.007.
Airway and breathing management skills are of paramount importance in the Emergency Department. This importance becomes even more significant during the resuscitation of the crashing trauma patient. Failure to efficiently manage the airway contributes to increased mortality and morbidity in these patients. Securing the airway in the setting of trauma, poses a considerable challenge in light of multiple other associated factors; like altered sensorium, shock, maxillofacial and spinal injuries or thoracic and neck injuries.
Rapid Sequence Intubation is the most widely used technique for emergency intubation of patients in the ED, with recent large registry data showing that it is used in 85% of all intubations in the emergency setting 1, 2.
RSI consists of three phases- Pre-oxygenation, Endotracheal tube placement and Placement confirmation. In the already compromised trauma patients, any delay in the latter two phases can lead to the worst outcomes. The efficacy and speed of intubation depends upon the skill of the clinician. Early confirmation of tube placement is crucial in order to prevent further compromise due to adverse events like oesophageal or right main stem bronchus intubation 3.
Various methods have been described for distinguishing between endotracheal and oesophageal placement of the tube, which include visual confirmation during laryngoscopy, expansion of the chest wall during ventilation, auscultatory method, capnography, and chest X‑ray.
The current recommended method for confirming correct placement of an endotracheal tube, as per ACLS guidelines [2015] is continuous waveform capnography, in addition to clinical assessment 4.
Capnography is the currently accepted gold standard method for confirmation of ET tube position but it has several limitations, especially in the emergency setting. As waveform capnography works on the principle of detection of carbon dioxide, this proves unreliable in the setting of shock which is a common presentation in many trauma patients. Also, there is a limited availability of ETCO2 monitors in most ED’s.
Recent studies have identified Point of Care Ultrasound as a potential method to confirm proper ETT placement 5, 6. POCUS is an easy, portable, non-invasive and inexpensive bedside imaging modality which has myriad applications in the field of Emergency Medicine. 7
The current study, a prospective randomized control trial, aimed at the utilisation of point-of-care ultrasound during RSI in trauma victims. It also compared the utility of POCUS versus clinical examination in detecting tube placement in these patients, though confirmation of placement in all was done by the currently accepted gold standard technique of waveform capnography. This helps the Emergency Physician in early identification of airway or breathing problems, such as hematomas, tracheal tears, pneumothorax and vascular injuries and to plan accordingly.
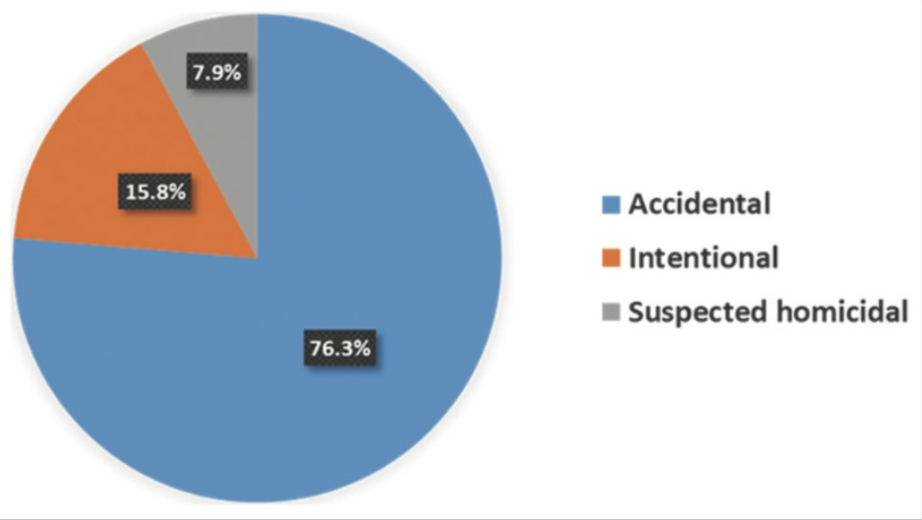
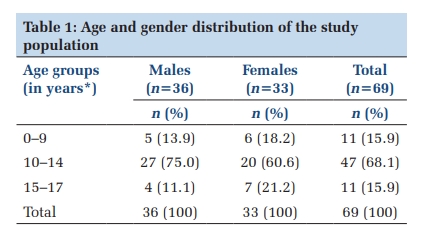
In our study, majority of the patients were males, which was similar to the other studies done by Chou et al, Mishra et al and Thomas VK et al6, 8, 9. Majority of our patients were in the 25-35 year age group and the most common mechanism of trauma was road traffic accident, which is in accordance with the WHO’s Injury and Violence Facts10 and also the findings of the study by Mishra et al 8. We found that the most common indication for RSI was airway protection, which correlated with the findings of previous studies 8, 9, 11.
Pre and post-intubation vital parameters of all patients of our study including Pulse Rate, Systolic Blood Pressure, Diastolic Blood Pressure and Saturation of Oxygen were found to be similar.
Mishra et al in a prospective randomized control trial found that during primary survey, without the aid of POCUS, there was a 3% incidence of clinical pneumothorax in the study population 8. This finding was comparable to our study which detected 4% of the study population.
In a prospective study by Kirkpatrick AW et al, using point of care sonography in a trauma centre, detected post-traumatic pneumothorax in 22% of the total population 12. Lichtenstein et al conducted a retrospective study and found that ultrasound was an effective bedside modality for diagnosis of occult pneumothorax, thereby reducing the need for computed tomography in a retrospective study 13. Nagarsheth et al conducted a prospective, single blinded study for identifying pneumothorax by ultrasonography as compared with CT and chest X-ray and found ultrasonography to have high sensitivity and specificity 14. During primary survey of the trauma populations with the aid of POCUS, Mishra et al found nearly 8% to have absent lung sliding which was suggestive of pneumothorax 8. This was comparable with the results found in our study. Additionally, we also detected the presence of neck hematoma in 1% of the population, which again correlated with the study findings of Mishra et al 8.
Wong et al conducted a prospective observational study in critically ill non-trauma patients, where they detected 4% to have an anticipated difficult airway 15. In our study, we found an anticipated difficult airway in 17% of the patients.
The mean time taken for the primary survey in the study conducted by Mishra et al was 20 seconds in the PA arm vs 18 seconds in the CE arm8. In our study, the mean time taken was 25 seconds vs 22 seconds in the PA and CE arm respectively. The difference was found to be statistically significant with a p value<0.001. Hence, usage of POCUS may prolong the time taken for primary survey, as compared to clinical examination alone.
Recent studies have demonstrated that the time needed to confirm endotracheal tube placement using POCUS ranged from 5 to 45 seconds16, 17, 18. Two studies compared the time taken using ultrasound vs capnography and found that ultrasound took shorter duration than waveform capnography 18, 19. Thomas VK et al underwent a prospective cohort study, concluded that ultrasonography method (8.27 ± 1.54 seconds) took significantly less time compared to clinical methods (20.72 ± 3.21 second) and ETCO2 detection (18.06s ± 2.58 seconds) for confirming tube placement (p-value <0.001) 9. Chou et al conducted a prospective, observational study and found that the time required for tracheal intubation confirmation using tracheal rapid ultrasound exam (T.R.U.E.) was 14.8±18.7 seconds 7. Mishra et al found that the mean time taken from the beginning of intubation to correct placement of the ET tube, and its confirmation by the presence of left lung sliding sign in the PA arm was 37.3 seconds (SD = 21.92). Similarly, the duration in the CE arm was 58 seconds (SD = 32.04)8. In our study, the mean time taken from the beginning of intubation till positive confirmation of tube placement was significantly lesser in the PA arm when compared with the CE arm (45.00 ± 7.83 seconds vs 91.36 ± 19.63 seconds, p<0.0001). From the above findings, it is evident that incorporation of POCUS into RSI of trauma patients leads to earlier confirmation of tube placement and this is a crucial advantage in the Emergency setting where time is of essence.
Mishra et al, in their study, found that 4% of the total intubations were oesophageal 8. In two separate studies conducted by Thomas VK et al9 and Reddy et al 20, 5 % of the total numbers were detected to be oesophageal intubations. A study conducted by Chou et al found 15% oesophageal intubations in the total population 7. In our study, we found that 5% of all the intubations were oesophageal.
The mean time taken to detect oesophageal intubation was 22 ± 2s in the PA arm of our study, as compared to 114 ± 5.65s in the CE arm with a statistically significant difference between the two (p< 0.0001) . Mishra et al found that the mean time taken to identify oesophageal intubation by using POCUS was 18.25 s vs 177.5 s taken to detect the same by clinical examination 8. Muslu et al conducted a prospective randomized control trial and found that POCUS could detect ET tube position in the trachea or the oesophagus in an average of 3 seconds 21. Several studies conducted during intubation found that POCUS had high sensitivity for identifying oesophageal intubations 21, 5, 16, 17, 22, 23, 24, 25, 26. From the above data, we can infer that POCUS can be used as a tool for rapid identification of untoward airway complications in RSI like oesophageal intubations.
Following the detection of oesophageal intubation in our study, the mean time taken for re-intubation was 26.67 ± 3.05 seconds in the PA arm and 55 ± 7.07 seconds in the CE arm and the difference between the two was found to be statistically significant with a p value < 0.007. Mishra et al found that in their study, the average time taken for reintubation was 23.12 seconds, when endotracheal tube placement was confirmed by the left lung sliding sign 8. When correct tube placement after reintubation was confirmed by EtCO2 value, the mean reintubation time became 39.5 seconds 8. As previous studies have already demonstrated the utility of POCUS in leading to faster confirmation of tube placement, it therefore also helps to hasten the process of reintubation and prevent further decompensation.
Point-Of-Care Ultrasound (POCUS) has emerged as the bedside diagnostic standard of care in trauma and emergency care settings. Recent literature reviews have shown the advantages of POCUS in airway management, especially for confirmation of correct endotracheal tube (ETT) placement as well as detection of oesophageal intubations.
This study demonstrated the feasibility and accuracy of a point-of-care ultrasound integrated RSI technique for trauma resuscitation. We found that POCUS is useful for detection of Airway and Breathing problems such as neck hematoma and pneumothorax during the primary survey at the time of pre-oxygenation. It shortens the time taken for RSI by more rapid detection of ETT placement, oesophageal intubation and correction of the same if detected.
The mean procedure time for ETT placement was less in the PA arm compared to the CE arm (45 vs 91.36 seconds, p<0.0001). Oesophageal intubations were detected in the PA arm in 22 vs 114 seconds in CE arm (p< 0.0001) and the time taken for effective reintubation was 26.67 vs 55 seconds in the PA and CE arm with a p value < 0.007 respectively. Statistical analysis revealed a significant difference between the two groups, in favour of the PA arm group.
Waveform capnography, chest X-ray and 5-point auscultation are all the conventional methods for identifying ETT position in trachea or oesophagus. Our study concluded that POCUS in RSI is non-inferior to any of the above methods and suggests that it may even be superior to the conventional techniques as it has a shorter mean time for confirming ETT placement as well as for detecting certain adverse complications of RSI such as Oesophageal Intubations.
Subscribe now for latest articles and news.